Latest News
- Clues beginning to emerge on asymtomatic SARS-CoV-2 infection
- Back in November of 2020, during the first wave of the COVID-19 pandemic, I was teaching an in-person microbiology laboratory. One of my students had just been home to see his parents, and they all c…
- Read more
- Could there maybe be better uses of genetics and probiotics?
- Professor Meng Dong and his laboratory have created a probiotic that can metabolize alcohol quickly and maybe prevent some of the adverse effects of alcohol consumption. The scientists cloned a highl…
- Read more
- ChatGPT is not the end of essays in education
- The takeover of AI is upon us! AI can now take all our jobs, is the click-bait premise you hear from the news. While I cannot predict the future, I am dubious that AI will play such a dubious role in…
- Read more
- Fighting infections with infections
- Multi-drug-resistant bacterial infections are becoming more of an issue, with 1.2 million people dying of previously treatable bacterial infections. Scientists are frantically searching for new metho…
- Read more
- A tale of two colleges
- COVID-19 at the University of Wisconsin this fall has been pretty much a non-issue. While we are wearing masks, full in-person teaching is happening on campus. Bars, restaurants, and all other busine…
- Read more
Chapter 14 - COVID-19
14 - 1 SARS-CoV-2, the virus that causes COVID-19

What is a virus?
Before we can talk about COVID-19, you need to understand some background about the virus, SARS-CoV-2 (COVID-19) is the name of the disease, SARS-CoV-2 is the name of the virus). And before you can do that, you need to understand the definition of a virus. A virus is not a living thing. It is more like a machine. It will have an outer shell, and within that shell is a small set of recipes that describes how to make a set of enzymes. This recipe book uses the same language that living things of this planet use: nucleic acids. These enzymes are molecular machines that, instead of doing useful work for the cell, pervert its functions and force it to make copies of the virus. Eventually, the virus leaves the cell, either by budding from the cell membrane or by killing the cell and causing it to burst open. The virus then spreads to other cells. Viruses are enemies of their hosts. If they are not dealt with effectively, they can lead to chronic damage to their host and, in the worst cases, death.
COVID-19 structure and replication
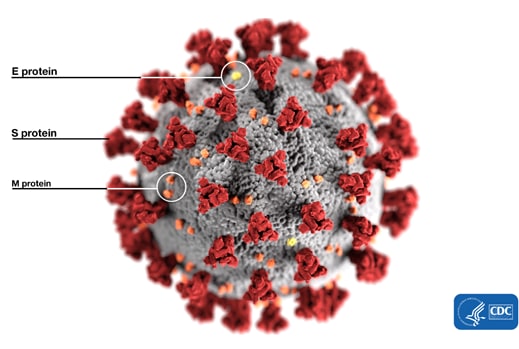
SARS-CoV-2 is one type of virus that infects humans; specifically, it is a coronavirus. A membrane decorated with several proteins surrounds SARS-CoV-2, with the spike protein probably being the most important for immunity. The prominent spike proteins give the virus the appearance of a solar corona, thus the name of the family (Figure14-1).

Figure 14.1. An artists depiction of the outside structure of the SARS-CoV-2 coronavirus. Note the ubiquitous presence of the Spike (S) protein on the surface of the virus. Image by Alissa Eckert and Dan Higgins from the CDC and is in the public domain.
{kind=link}
Your genes, which determine all your capabilities, are encoded in DNA. Some viruses do an interesting trick in that they don't use DNA for their genomes, but instead use RNA. RNA is another type of nucleic acid that can encode information, but it does not store hereditary information in living things. RNA is unstable, and, if used in our chromosomes, too many genes would mutate and be lost. However, coronaviruses do use RNA as their genetic material, and they appear to be able to get away with it since they continue to exist. These viruses contain a single strand of RNA that is about 30,000 bases long. A strand of nucleic acid that long is pretty big for an RNA virus (there are lots of other RNA viruses in the world, but they tend to be about 10,000 bases or less). One of the genes encoded by this RNA is for an RNA replicase that can copy the viral genome. Your host cells do not have an enzyme that is willing to copy RNA into RNA, so the virus has to provide its own. The large RNA replicase is unusual in that it encodes a proofreading ability, which is probably necessary given the large size of the virus. Because of this editing capability, these coronaviruses don't change as quickly as other RNA viruses, such as the influenza virus.
SARS-CoV-2 enters cells by attaching to the ACE2 (angiotensin-converting enzyme 2) protein. ACE2 receptors are common on epithelial cells that line the lung, heart, kidney, brain, and gut, thus accounting for the widespread infection of different organs. Once SARS-CoV-2 binds, the cell then takes up the virus. Why in the world would the host cell willingly do this? That is one of the many clever things viruses do. To enter cells, viruses take advantage of material transport pathways in the host. SARS-CoV-2 hitches a ride on the endocytotic pathway in human cells. The host cell engulfs the virus in a membrane, called an endosome, that floats like a little bubble inside the cell. From there, the virus's entry into the cytoplasm depends upon acidification of the endosome, cleavage of the spike protein by the host, and a conformational change. When all this happens, a membrane fusion between the viral envelope and the endosome occurs, and the nucleocapsid then enters the cytoplasm. When the coronavirus genome enters cells, it pretends to be something called a messenger RNA. mRNAs are copies of genes headed to the protein factory of the cell, the ribosome. The ribosome will translate the recipe encoded in a mRNA into a protein. Thus, the SARS-CoV-2 RNA fools the ribosome into translating it into viral proteins. These viral proteins make copies of the viral RNA, form into the spike, E and M proteins, and perform other various functions for the virus. After enough copies of the virus and viral proteins are present, they will assemble at the host membrane, and new virions then bud from the cell. These viruses then go in search of other cells to infect.
14 - 2 Origins, spread, and risk of COVID-19
Where did it begin?
There is significant controversy about the source of the COVID-19 outbreak. Currently, the earliest known existence of a virus resembling SARS-CoV-2 came from samples harvested from Dead Pangolins brought to the Guangdong Wildlife Rescue Center of China on Oct 24th, 2019. The government of China monitors wildlife to sound the alarm if a potential pandemic strain is detected. Patients ill with viral pneumonia of no known cause began to appear in December in Wuhan, China. The first case was diagnosed on Dec 1st in China and had no apparent link to the market. There were another 41 cases, with 28 associated with the wet market in the city. However, 13 of 41 did not visit the market.
Bats are a known reservoir for these types of viruses. Pangolins are probably not the original source of the virus but were an intermediary host that was infected both with a pangolin coronavirus and a bat coronavirus. As these viruses grew in the pangolin, there was a chance to exchange genetic material in a recombination event, creating the deadly pandemic strain. How did this then make the jump to humans? It appears that the genetic changes to the spike protein of coronavirus made SARS-CoV-2 able to bind to the ACE2 receptor of humans where the parent strains it arose from could not. One hypothesis is that the virus made the jump to humans from a dead pangolin, bat, or other animal. A person that was then ill with COVID-19 entered the market and spread it to others.
How did it start spreading?
The first infection was probably a poor fit between the SARS-CoV-2 strain and the ACE2 receptor of the human host. But, as the virus grew, mutations in the spike protein would occur. Those that had a better fit to ACE2 would have a selective advantage. Thus, the more the virus grew in humans, the more adept it became at infecting them. As it moved from host to host, the efficiency of transmission and replication probably increased. This adaptation of SARS-CoV-2 is not unique. All viruses change and sometimes these changes allow them to infect new hosts.
Why is COVID-19 more deadly?
Coronaviruses have infected humans for millennia, typically causing a mild upper respiratory infection we refer to as a cold. (There are several classes of viruses that cause cold-like symptoms, coronaviruses are just one of them.) Why is SARS-CoV-2 different? In contrast to many viruses, the receptor used and the binding process of coronaviruses vary considerably across each coronavirus variant. The receptor target dictates the host range and tissue specificity. SARS-CoV-2 uses the ACE2 receptor where other, less damaging coronaviruses do not. Using ACE2 gives the virus access to the lungs, heart, kidneys, brain, and gut. As the body fights the infection, it will cause inflammation and damage wherever the virus is growing. As the lungs are damaged, they fill with fluid, causing pneumonia and shortness of breath. If the heart is involved, heart failure and cardiovascular events occur. Infections in the gut cause diarrhea. COVID-19 can cause all of these symptoms.
What are the risks of infection?
Everyone appears to be a target for the virus. Recent statistics from the Wisconsin Department of health show the breakdown of infection rates for every age group (Figure 14-2) Not everyone who has COVID-19 is going to experience life-threatening symptoms. Results from an analysis of over 72,000 cases in China paints a clearer picture of the risks of COVID-19 illness. The majority of people (81%) who get infected with COVID-19 will have mild disease, about 14% of cases will cause severe disease, and 5% of cases result in critical infection. Half of the patients who become critically ill do not survive. The death rate of diagnosed cases appears to be between 2.5-5%. Still, most countries are probably undercounting the number of actual cases, either because people are not seeking medical attention or from a lack of testing capacity.

Figure 14.2. Age distribution of those infected by SARS-CoV-2 in Wisconsin. Anyone can contract COVID-19. The higher rates of infection in those older than 20 years old is probably because the illness can be more severe and those patients will seek treatment. Those younger than 20 were probably not as readily tested for the illness. Data taken from the Wisconsin Department of Health.
Why do some people appear to have little to no symptoms, and others struggle with this disease to such a large degree? We are getting a better understanding of important factors that affect the outcome. Your risk of dying from COVID-19 depends significantly on your general health. First and foremost, no one's risk is zero. Previously it was thought that children under the age of 9 did not develop severe illness. However, the state of New York has identified 102 cases of pediatric multi-system inflammatory syndrome caused by SARS-CoV-2 that can be fatal if left untreated. As age increases, the death rates increases, Figure 14-3, but this has more to do with the accumulation of health problems.
The strength of your immune system and its ability to get the infection under control also seems to play an important role. If the virus can replicate to high numbers, it can spread systemically. Viral sepsis, probably by COVID-19, is a strong predictor of adverse outcomes. It appears that if the virus spreads into the cardiovascular system, it may cause damage to the heart and to blood vessels since these cells have the ACE2 receptor. Inadequate organ function due to the infection or pre-existing health conditions is a strong predictor of poor outcomes.

Figure 14.3. Who dies from COVID-19. The figure shows deaths for each age group and the increase in risk for each pre-existing condition. As age increases the death rate also increases. This has more to do with how many preexisting conditions a person has than their age.
The US is at greater risk for complications from COVID-19 infections because the CDC estimates that 45% of the population has at least one of the pre-existing conditions mentioned above. Seven behaviors contribute to the likelihood of complications: smoking, sedentary lifestyle, obesity, diabetes, hypertension, high cholesterol, and inadequate fruit and vegetable consumption. In other words, our bad habits as a society are about to exact their revenge on the population as a whole thanks to COVID-19. If you have one or more of these pre-existing conditions you need to be extra careful to try to avoid COVID-19.
Is the death rate from COVID-19 accurate?
Due to the lack of testing and the inexperience of health professionals dealing with a pandemic, it is highly likely that the number of COVID-19 deaths early in the pandemic was inaccurate. Some argue deaths are being incorrectly attributed to COVID-19, while others claim the situation is leading to an undercount. To answer this question, the CDC did a study of excess mortality in New York City. NYC was an early epicenter of the epidemic, having thousands of active cases. The NYC health department previously developed an electronic vital statistics reporting system that provides a rapid and nearly complete count of all deaths in the city. Using this database, researchers were able to compare the all-cause mortality in NYC in previous years with mortality in the current year. By subtracting a baseline expected death rate, it is possible to calculate the number of excess deaths in 2020. From March 11–May 2, 2020, a total of 32,107 deaths were reported in NYC, which is 24,172 deaths above the expected baseline. Subtracting all reported COVID-19 deaths during this period leaves 5,293 excess deaths. Most of these are probably due to COVID-19, but not all. Some may be from patients who fear or could not seek medical attention due to the epidemic but were not infected with the virus (for example, someone having a heart attack). The large number of excess deaths is compelling evidence that health departments were underestimating the death rate from the epidemic by up to 22%.
Since vaccinations have become available, the situation has probably resolved, and COVID-19 deaths are now being accurately recorded. This is partly due to a better understanding of COVID, but also due to the lower death rate since more of the population is vaccinated. However, far too many people (379 a day in the US in July 2022) are still dying of COVID.
14 - 3 Various responses to COVID-19
How to stop the spread of COVID-19
A virus spreads in society because those ill with the virus make contact with others who are susceptible. If the virus transmits to more than one other person for each person it infects, it will cause an epidemic. This ratio is called the reproduction number and is denoted as R naught (R0) by epidemiologists. Each infectious disease has a base-line R0 that indicates how well it naturally spreads in a population, but it is possible to alter this number by changing behavior. For example, it appears COVID-19 has a maximum incubation period of about 14 days. If it were possible for everyone to stay home for three weeks (just giving a buffer here) and never make contact with another person, R0 would go to zero. Of course, this is an extreme example. Modern society cannot function without any human interaction. But it does demonstrate that changing human behavior can slow the spread of the virus. As the virus has spread around the world, various countries have tried different measures to stop the spread of COVID-19. In this section, we will examine several successful examples and one poor example currently unfolding.
China's response to the virus
Initially, China attempted to suppress information about a new type of pneumonia that was popping up in Hubei province. The first case of COVID-19 may have occurred as early as November 17th, 2019, and Chinese authorities tracked at least 266 people who contracted the virus in that year. The Chinese government attempted to hide information about the virus, even punishing doctors who tried to warn their colleagues about a new SARS-like virus that was spreading in the City of Wuhan. To be fair, the initial emergence of a new infection is often mistaken for other diseases, and it is only in hindsight that disease origins become apparent. However, the punishing of physicians trying to raise the alarm suggests a more sinister purpose. Authorities in China finally recognized the virus and reported on January 21st that there was host-to-host transmission of COVID-19.
Once China confronted (or admitted) the growing epidemic, how did they limit the spread of the virus so that only about 84,000 cases occurred? (Note: I doubt the reported cases in any country are the actual real cases due to either inadequate testing or inaccurate reporting of incidents). First, China had a plan in place. Planning is essential to the response to any crisis. Knowing what you are going to do before a crisis hits allows the identification and preparation of equipment and personnel that will be needed. It is much easier to get resources in place beforehand than to attempt to do it during a crisis. Marshaling resources in a time of crisis is always tricky because of the compressed timeframe.
As the seriousness of the epidemic became clear, China implemented a quarantine beginning on January 23rd, eventually encompassing all of Hubei province, putting 45 million people under stay-at-home orders. The government suspended all public transportation, and large gatherings were prohibited. Community committees delivered needed food, medicine, and medical supplies to residents, reducing the need for outside trips. Two emergency field hospitals with 2,400 beds were constructed within a couple of weeks to house those with severe cases of COVID-19. Large venues were transformed into medical observation and treatment centers to accommodate less ill patients. These could support up to 14,000 people. The deployment of medical rescue teams from other areas of China to Hubei ensured enough personnel to staff these treatment centers. Having space to isolate all COVID-19 patients decreased the spread of the disease in the community.
A grid-closed management system prevented unnecessary interaction of individuals. The policy restricted movement, allowing only one person outside to run errands every two days. Each area was closed off, with only one entrance and exit point, facilitating close monitoring of movement. As each person traveled through these grids, they had to scan a QR code. Thus anyone who tested positive could be rapidly identified, and all their contacts quickly traced. This draconian monitoring is a significant invasion of privacy. There are better-designed applications that protect privacy, but allow the same ability to trace contacts (see below). Some of the methods to encourage compliance involved beatings and near imprisonment. These types of responses are extreme and unwarranted. On January 27th, all schools were closed, and instruction went online. Outside of Hubei, all passengers underwent temperature tests at airports, railway stations, and bus stations.
In the economic sector, aggressive measures prevented business failures and helped the medical response during the epidemic. Lower loan thresholds and loan rates allowed businesses to borrow money under more favorable terms. Companies could also apply for tax relief and other government funds to help them survive. Some businesses shifted production lines to produce medical protective equipment and ventilators. China has the manufacturing capacity to do this.
The epidemic is now better controlled within China. To prevent reinfection from abroad, entering flights are restricted to twelve airports, and incoming passengers must undergo COVID-19 testing and quarantine until results come back negative. The aggressive measures taken by China limited the spread of the virus, and new cases of COVID-19 began to decrease within two months. Today, the Chinese government reports that there is no sustained spread of the illness within the country. Hopefully, this success can continue, and again, one should treat the reports from a historically secretive country with skepticism.
China continues to monitor the virus and impose strict lockdowns when infection rates begin in an area. This policy has been successful in controlling the virus and keeping deaths low. As of July 2022, they have recorded 14,647 deaths, much less than many other countries. There is some concern that the reporting coming from China is not accurate.
In hindsight, China's zealous response to the virus may have gone too far. Their zero-COVID policy repressed the virus for years, but in the interim, their population did not vaccinate completely. The inactivated vaccines that China developed, CoronaVac and Sinopharm, provide strong protection after three doses. Too many in the Chinese population did not get three doses, and because of this, when China relaxed the zero-COVID rules late in 2022, infections exploded. The CDC estimates that from December 2022 to February 2034, 1.41 million died in the ensuing wave. Repression of the virus caused significant psychological and economic damage. However, for those who did get vaccinated, they were protected from the illness. The high death toll was caused by a lack of progress in vaccination.
Taiwan's response to the virus
Because of its proximity to China and the previous SARS epidemic of 2003, Taiwan centralized its emergency response to outbreaks by creating a new agency, the National Health Command Center. The NHCC had broad authority to organize the response and to advise the government on appropriate steps. On December 31st, 2019, when China notified the World Health Organization of a viral pneumonia of unknown origin, the NHCC began to act. Taiwanese officials started to board planes that were direct flights from Wuhan and assess passengers for fever and pneumonia symptoms. Any individual with symptoms has to place themselves into quarantine. On January 5th, authorities expanded monitoring to any individual who had traveled to Wuhan, China, not just direct flights. By January 20th, an organized government response involving at least 124 separate items began including border control from the air and sea, case identification (using data and technology), quarantine of suspicious cases, contact tracing, resource allocation, reassurance and education of the public while fighting misinformation, formulation of schools and childcare policies, and relief to businesses.
Why was Taiwan's response so effective? The most critical factor was the speed of the reaction. Within days of being notified of an outbreak in China, Taiwan took aggressive steps to identify potential cases of the new illness. Second, a coordinated response against the virus at the national level enabled the entire society to work together. Third, the leveraging of information and technology helped to identify and contain cases rapidly. For example, within one day, the national health records database was integrated with the national travel database, allowing doctors to immediately know the travel history of any patient coming to their office. Also, citizens who entered quarantine were tracked on their phones and received emotional and financial support, including meals, to ensure they stayed home. This comprehensive response prevented the establishment of the illness in Taiwan. As of May 23rd, there have been 441 cases of COVID-19 and seven deaths.
South Korea's response to COVID-19
South Korea is a close neighbor and trading partner of China. Because of the frequent travel of tourists, workers, and academics between the two countries, it was inevitable that COVID-19 cases would ultimately spread to South Korea. Instead of a nationwide lockdown, South Korea focused on rapid and widespread testing facilities and aggressive contact tracing. A vital element of the contact tracing was the rapid development and distribution of apps that helped discern contacts of COVID-19 positive patients. The first confirmed case of COVID-19 entered South Korea at Incheon International Airport from Wuhan, China. The individual was discovered after a temperature screening and immediately tested for the virus. The government quickly reacted, increasing its alert level from Aware to Care and released information about the patient's movement to alert the public of any possible exposure. Korea began to monitor all travelers coming from China and opened screening centers to detect asymptomatic carriers. The government prepared local hospitals as infection control institutes, and anyone testing positive was placed under quarantine and their contacts traced. Authorities also monitored all discovered contacts to prevent further infections. In early February, the number of COVID-19 patients grew steadily, and the government expanded testing to even marginal contacts with known COVID-19 positive cases. The government quickly approved further kits to test for the virus, facilitating the expanded testing. By February 28th, laboratories were able to conduct 15,000 tests per day. Tests were free for all residents, and as of March 16th, the Korean government had tested 250,000 people.
On February 19th, surveillance identified the 31st patient and discovered her to be the origin of a super spreader event. This individual had close contact with many in a church congregation and ended up spreading the infection to thousands of individuals. The government began limiting trips and outdoor activities and imposed emergency safety measures such as basic hygiene rules and social distancing. Drive through testing was first suggested by Jaemyung Lee, the governor of Gyeonggi Province. He observed that one-on-one testing had limited ability for social distancing, put health workers at high risk, and consumed large amounts of PPE. Low-contact drive through testing solved these problems, allowing safe testing in 10 minutes or less. Patients could learn the results of their tests via a text to their phone in three days or less. Due to the rapid deployment of testing centers, it was initially difficult for the public to locate them. To help solve this problem, the maker of the OilNow app, which usually locates the nearest gas station, added a service that mapped all testing centers.
Those in densely populated areas may not have cars or space may not be present to implement drive-through testing. In these areas, walkthrough centers enabled testing of patients from booths equipped with depressurizers (to prevent the spread of infectious virus), intercoms, and attached gloves that allowed doctors to interact with and collect samples from patients. The patient stands outside the booth, and the physician inside performs testing procedures. Daily counts of tested, positive, in quarantine, out of quarantine, and deaths appear at a website that was available to the public. Citizens could drill down into the information looking at all positive tests in their neighborhood, along with individual movement trajectories of COVID-19 positive cases in their area.
Contact tracing in South Korea is more straightforward because each mobile phone account links to a national ID. Combining this tracking data with credit card transaction history, and video footage from public surveillance cameras made it possible to reconstruct the movements of positive COVID-19 cases in great detail. Health authorities targeted contacts of cases for testing and precautionary self-quarantine. The Korean government developed this aggressive form of contact tracing with health emergencies such as the current pandemic in mind. Due to pressure by citizens, the government released this information to the public. Widespread distribution of this information has helped residents understand their risks, avoid hot spots of infection, and decide whether to be tested. Transparency is almost always the best course of action. Authorities used text messaging information systems, initially designed to inform citizens in local areas of disasters, to keep the public informed. General messages were sent to all residents every day to inform them of the number and location of cases in their area. Specific texts were also sent to individuals if their paths had crossed with a known COVID-19 positive case. Some found these frequent contacts overwhelming, but overall it was well received. Armed with the movement data, several private companies developed applications and websites that could trace the user's paths compared to those who were COVID-19 positive. The translation of mapping data into a visual, interactive form made it easier for citizens to modify their behavior. Some apps even alerted the user when they were within 100m of a confirm patient's trajectory.
All residents and visitors to Korea are required to install a mobile app developed by the Ministry of Health and Welfare. This app requires travelers to report potential symptoms for 14 days. If signs of respiratory distress or fever occur, the user must report to local health authorities for evaluation. As of April 1st, all incoming, long-term residents must self-quarantine for two weeks. The Ministry tracks quarantine compliance with the app.
As the number of cases grew in Korea, the government developed a smart management system to speed up contact tracing. Rapid tracing required the combination of data from the police agency, three telecommunication firms, and twenty-two credit card companies. The app was able to reduce the time consumed for contact tracing from one day to ten minutes. People exposed to a known COVID-19 case had to self-quarantine, and the government monitored their symptoms and location for 14 days using another mobile app. Unlike the travel tracking application, this application is voluntary.
South Korea was able to respond so rapidly to the COVID-19 epidemic because they had planned for years for such a possibility. The previous outbreaks of SARS and MERS made it clear that a worldwide pandemic was likely to occur in the coming years. Debates pitting privacy rights and sharing of customer data against public health already happened, and a balance was negotiated beforehand, saving valuable time.
One drawback of the Korean plan, as with the Chinese, was a significant intrusion into the private lives of its citizens to allow effective contact tracing. Other societies, such as the United Kingdom, the US, and Canada, may not be so willing to give up these privacy rights. Fortunately, there are other compelling solutions to contact tracing. (see below)
America's response to the virus
Before I begin this section, I should warn those who are fans of the federal government response that this assessment is going to be quite critical. This response was so outside what was expected that the medical journals, the New England Journal of Medicine and the British Medical Journal wrote editorials on it. A very unusual response. We must honestly face the mistakes made and the advice that was ignored if our society is going to learn and fight this epidemic productively. If reading about this timeline is going to upset you, you may want to skip this section. However, I encourage you to read it with an open mind.
The crisis in the US was an avertable catastrophe. President Trump willfully ignored numerous warnings from officials in the early months of 2020. On January 23rd, the World Health Organization warned all governments to get ready for coronavirus. Be prepared for active surveillance, detection, isolation of cases, contact tracing, and prevention of spread. After the first initial case arrived in the US on January 22nd, two months of inaction followed, with Donald Trump issuing false reassurances to the nation. China's efforts to combat COVID-19 slowed the spread of the disease and gave the US time to react. Fear of the political and financial consequences delayed the response to the pandemic. We could have increased the production of personal protective equipment, ramped up testing capability, expanded hospital capacity to deal with an influx of patients, and established transparent chains of command between states and the federal government. Afraid that it would spook the stock market, none of this was done.
Not only did Donald Trump not respond to the actual pandemic, his administration actively dismantled the government's preparation. Most of the participants in the pandemic preparedness drills the outgoing Obama administration put on for them have left. The disbanding of the White House Global Health Security office, the elimination of a global early warning system, PREDICT, that identified viruses of pandemic potential, the removal of a CDC expert in China whose job was to monitor outbreaks such as COVID-19, and cutting funding to critical programs at the CDC have all contributed to our governments lack of preparedness.
As the pandemic storm washed across the US, governors were left fending for themselves. The CDC had to resort to advising the use of bandanas as a substitute for PPE, and states competed in bidding wars to secure necessary equipment. The CDC made a critical mistake in designing a different test kit instead of using the one developed by WHO, which wasted valuable time. Stuck with a lack of testing and no ability to trace the contacts of those who tested positive, a large number of states and localities had no choice but to use the blunt instrument of stay-at-home orders for the entire population. Governments ordered citizens to enact social distancing, limit travel, avoid gatherings of ten or more people, and close non-essential businesses. These measures have met with variable success. Citizens of some states have observed these recommendations (NY, WI, CA), while others left open spring-break beaches, schools, daycares, and other non-essential activities, allowing the continued spread of the virus.
The US's patchwork response contrasts sharply with the coordinated response of Taiwan, South Korea, and China to the pandemic. Poor leadership at the federal level is the primary reason that the US was the epicenter of the epidemic in 2020-21, with tens of millions of cases and millions of deaths. Even more frightening is the irresponsible, premature push at the federal level to relax state health orders that, where implemented, have significantly slowed the spread of COVID-19. A rushed "return to normal" risks allowed the virus to again spread in communities, causing illness, death, and economic disruption on a scale not seen anywhere else in the world. The disappointing news that some states may manipulated their numbers is terrifying.
The anti-scientific pronouncements by Donald Trump have made matters much worse, from declaring that the pandemic would disappear on its own (2/28) to prematurely promoting hydroxychloroquine as an effective treatment (3/21). Panic buying of hydroxychloroquine ensued, increasing prices and leading to overdoses. Lupus patients, for which hydroxychloroquine has proven benefits, were unable to fill prescriptions. On the day the CDC announced that masks would help stop the spread of the virus, Trump said he refused to wear one. The penultimate level of ignorance was displayed when Mr. Trump suggested using disinfectants inside the body or UV light treatment of blood might be usable against coronavirus. Experts and companies that made disinfectants rushed to warn the public against inhaling or ingesting bleach products. In late April, Trump's arguably most extreme act was the call for large public protests against governors (conveniently from the Democratic party) for their stay-at-home orders. Mass groups of protestors exposed themselves to the potential spread of the virus, further exacerbating the situation and potentially leading to extended stay-at-home restrictions. Recent data indicates that 72 people likely contracted COVID-19 after attending a rally in Wisconsin protesting the stay-at-home order. So far, the US response at the federal level has been chaotic at best.
The premature reopening of economies in the Southern United States, promoted by Donald Trump and misinformed governors that are hostile to science, has created the crisis that experts predicted. As of July 12th, 2022 new cases in Florida (317,039), Georgia (105,303), Arizona (83,699), and Texas (288,520) indicate a virus raging out of control. Mandatory mask orders and reimplementation of restrictions could have brought the epidemic back under control, but mixed messages at the federal, state, and local level leave populations confused. In addition, propaganda broadcast from websites and news channels makes matters worse. The general population needed to educate themselves, start wearing masks, and social distancing. However, with the contradictory information coming to them from all sides, the general population is understandably confused.
A change of President has helped the US response. However, much of the damage has already been done. Over 1 million Americans have died from COVID-19, making it the 3rd leading cause of death. The vaccination campaign greatly decreased the spread of the epidemic, but because of misinformation, many citizens are afraid to be vaccinated, and we did not achieve herd immunity in a timely fashion. In fact, we are still not there, and I fear we never will be.
14 - 4 Stopping COVID-19
So we clearly dropped the ball on this infection. Our constitution is a primary difference between the United States and governments that have been more successful in dealing with the pandemic. In the United States, due to its constitutional structure, the primary responsibility for public health rests with the states. In the ordinary course of daily life, this is not a problem, but in extraordinary times, such as a global pandemic, decisive national action is necessary. States and the federal government can activate emergency powers to expand their ability to protect the life and health of citizens.
When enacted, the resulting emergency government powers are sweeping, including halting business operations, restricting freedom of movement, limiting civil rights, and commandeering property. A primary concern with these orders is the state overstepping their authority when it is not necessary. However, in the COVID-19 epidemic, we have the opposite problem: the federal government has done too little. What should our society and our government learn from other countries' successful mitigation efforts? Here are some possible suggestions.
- First, the stay-at-home orders need to continue until infection rates drop for at least 14 days. We need to get the incidence of infection low enough in the community that the risk of transmission to the still mostly susceptible population is small enough to allow more interaction between people. I do believe that these orders need to be more sharply focused. It is nonsensical for counties where there are only a few cases to be locked down because other areas of the state are seeing large numbers of infections. The one major caveat to this is that testing must be available so that there is an accurate assessment of the spread of COVID-19.
- Everyone in the population, when out in indoor public spaces, needs to wear a mask. A recent study models the effect of wearing a surgical or homemade mask while in public spaces. There is also an excellent press article about the research. These scientists do a careful analysis and build a model to determine the effect of wearing a mask on the spread of the infection. Many different types of masks will work, including cloth ones. If 80% of a population begins wearing masks before day 50 of an epidemic, it can bring the infectivity rate low enough to stop the spread of disease. The most important effect of wearing a mask is preventing those who are sick from spreading it to others. In other words, wearing the mask protects others, not you. However, if everyone does it, the spread of the diseases becomes unsustainable. One of the most important findings of the model was that mask-wearing is more effective than stay-at-home orders. Most parts of the US are still in the early days of the epidemic and can implement this plan. I worry, however, that too many Americans will not follow this advice.
- Testing has to increase to the level that anyone who needs a test can get tested. Testings must include routine surveillance of all healthcare workers, anyone with potential symptoms, and their recent contacts. Tests must be available to everyone who fits the case description of COVID-19, not just those with severe illness. Widespread testing will give a better understanding of disease incidence. The good news here is that testing capacity in the US is increasing and surpassing the need in some places. For example, Wisconsin currently can perform 15,000 tests a day, yet doctors are only ordering 3,000 to 4,000.
- Ideally, those with moderate illness should be quarantined in locations away from others. While self-quarantine is possible for those who have enough room in their homes, patients in crowded living conditions (e. g., dorms, apartment buildings, prisons) need to have alternative accommodations to prevent the spread of illness.
- A contact tracing mechanism must be developed and deployed. The ones used in China and South Korea are probably not compatible with the attitudes and laws about privacy in the United States. However, groups are developing other solutions that can achieve the same goal without the invasion of privacy the current solutions entail. Both Apple and Google announced that their phones would have this capability by mid-May of 2020. Unfortunately, a misguided obsession with privacy rights, in my opinion, is polluting this effort. Both Google and Apple are refusing to allow these apps to record locations so that detailed routes and times of ill individuals can be cross-matched against others. This kind of detail is essential for public health departments. It is especially ironic considering the massive amount of information Facebook and Google collect on users of their systems.

Figure 14.4. Contact Tracing App. The contact tracing application depends on the ability of phones that are adjacent to each other to communicate. This interfacing enables your phones to keep track of your contacts with pinpoint precision.
If we had implemented these five steps, we could have bought more time for scientists to develop effective treatments and, eventually, a vaccine. Marcel Salathé (an epidemiologist) & Nicky Case (a programmer and artist) lay out a compelling case to guide the future reaction. I encourage you to read their analysis. Our country acted too late to take advantage of many of these measures. However, the rapid development of vaccines helped to protect people from serious illness and death for those who took them.
14 - 5 Treatments for SARS-CoV-2
What are potential treatments?
There is an understandable keen interest in potential treatments because of the increased risk of death from COVID-19 compared to other infectious diseases. The public and news media are looking to scientists to find remedies, and any drug that shows promise gives rise to intense publicity. Finding and testing effective treatments is a complicated and time-consuming business. Many journalists and the public at large do not have the necessary training to judge the validity of studies published in the literature or the background to evaluate appropriate controls, randomization, and all the other subtle nuances that go into a well-designed drug trial. This inexperience can lead to misinterpretation and overhyping of preliminary results. It doesn't help that some physicians who run these trials do not design good experiments. The skillset for being a doctor, where you are trying to diagnose what is wrong and treat illness effectively, is very different than that of a scientist doing research. It's not that doctors can't be great scientists, many are. It's just that being a great doctor doesn't automatically mean you have an inclination for research.
The efficacy of potential drugs against the SARS-CoV-2 virus are often first tested against the virus in cell culture. It is possible to grow human cells in special liquids that will support their growth. Scientists then expose the cells to the virus and then observe the life cycle of infection in the presence and absence of test drugs. If a drug slows or stops the progress of SARS-CoV-2, it merits further study.
Testing of SARS-CoV-2 in animal models is often the next step. Scientists are rapidly evaluating several animal models to see if they can support the growth of SARS-CoV-2. Potential animals include mice, rats, hamsters, and monkeys. The news that cats can be infected and develop observable disease makes them another possible model. Because of the urgency of finding effective treatments, some drugs will move directly into human trials.
Just because a drug can stop a viral infection in the test tube does not mean that it will do the same thing in an animal model or a human. The drug may be toxic to humans at the level needed to affect the virus. Side effects from the drug may also be too severe to allow its use. Also, the drug may not be absorbed by human patients and will not make its way to sites of infection in the body. These are just some of the reasons a promising drug in the lab may not be effective when administered to a human.
With these caveats, this section explores what drugs have made it to clinical trials and what the future might hold. Treatments for COVID-19 are a moving target, and this section highlights the most recently reported results. As more information becomes available, this section may become out of date.
What's up with hydroxychloroquine?
The case of hydroxychloroquine is a perfect example of what can happen in the process of a drug trial. Chloroquine and hydroxychloroquine have antiviral properties. In late January, Wang et al. reported that initial cell culture experiments demonstrated an inhibitory effect of chloroquine against SARS-CoV-2 at dosages appropriate for humans. Because of their findings, the authors recommended drug trials in patients should begin immediately.
On March 20th, 2020 Gautret et al. reported clinical trials with hydroxychloroquine with or without azithromycin. After six days of treatment, 15% of control patients had cleared the virus, while 70% of patients taking hydroxychloroquine were virus-free. When combined with azithromycin, all patients had cleared SARS-CoV-2 by day 5. There were several problems with this study. First, the sample size was small, enrolling only 36 patients. Second, the patients were not randomly assigned to each group, and they were not balanced by age, pre-existing conditions, sex, and other variables that are known to influence outcomes. Finally, the test was open-label, meaning patients and doctors knew who was getting treated with a drug and who was not. Still, the treatment showed promise and warranted further investigation.
A second clinical trial at about the same time by Chen et al. appeared to support the use of hydroxychloroquine. Patients were assigned randomly to a test or control group, the control group received a placebo, and both the attending doctors and patients were unaware of the group assignments. After five days, the test group's fever disappeared 2.2 days earlier, coughing ended sooner, and chest CT scans showed that 80% of the patients had improved compared to 52% in the control group. The main criticism of this study was that it was small, having only 62 patients, but again, further investigation was warranted given the significant, positive results.
On May 11th, 2020 Rosenberg et al. published a study looking at the success of treatment with hydroxychloroquine with or without azithromycin. In contrast to earlier work, this was a large study of 1,428 patients. In their work, the scientists looked at mortality in patients and found no significant benefit of treating them with these drugs. One drawback of this study was its observational design. Instead of assigning patients as they entered for treatment, this study only collected the records afterward. There was no opportunity to assign patients to control and test groups randomly. The study did suffer from flaws because those in the test group were more likely to be male, have cardiovascular disease, or diabetes. All of these are known to result in worse outcomes. Also, the patients and doctors knew they were receiving treatment. However, if hydroxychloroquine and azithromycin were having a profound effect, it should have been picked up in this study.
How can a drug seem to show promise in some studies, and then not have any success in others? It has to do with the design of the study, uncontrolled confounding variables, and the number of participants. First, knowledge of the patient and the doctor to your treatment can have a powerful effect. If you believe you are getting something useful, you will feel better, at least for a while. Your attending physician may also have an unconscious bias because they know you are in the treatment group. This bias is what is called the placebo effect. A well-designed study will blind participants to their group assignment to neutralize this phenomenon. Second, a control group is necessary for any quality research, and it needs to have identical conditions to the test group, except for the drug under study. Third, balancing the overall health of the individuals in each group is also essential. For example, if the control group has more patients with pre-existing conditions, they will likely have poorer outcomes. Finally, the number of patients in the study has to be large enough that it is possible to see statistical differences between each group. All of the early studies had significant design flaws, and so did the last one, but it was the best of the bunch. If hydroxychloroquine has substantial clinical benefit, it should have shown up in this last large study.
Unfortunately, the politicization by the president and his detractors of the legitimate research on hydroxychloroquine is unhelpful. There is indeed no strong evidence for the use of hydroxychloroquine for the treat of COVID-19. However, the comments by detractors of the president who, in my opinion, are exaggerating the risks of taking hydroxychloroquine are equally misinformed. The drug does indeed have serious side effects, and recent studies have demonstrated that the risks, including heart abnormalities, heart failure, and death, outweigh any benefit. These side effects are rare, and hydroxychloroquine has been used for decades to treat malaria and lupus. In any case, no one should be taking the drug unless under the supervision of a physician.
Remdesivir
Remdesivir is another drug that showed promise in that first initial study by Wang et al. cited above. Several clinical trials around the globe have tested the success of remdesivir against Sars-CoV-2 infection. As with hydroxychloroquine, some studies suggest positive effects, but in most cases, poor experimental design makes them hard to interpret.
A report by Antinori et al. is an excellent example. Physicians are desperate to try anything that might help. Patients are given drugs without including control groups. In the face of a deadly illness such as COVID-19, using control groups is fraught with ethical problems. If a drug turns out to be effective, harm was done to those who died in the control group. However, the absence of a control group makes it difficult to determine the efficacy of any treatment. The results of the study show that only 38.9% of those in the ICU had improved, while 44% died. However, this is better than reports from Northwell Health in New York, where 88% of patients on mechanical ventilation had died.
A notable finding from Antinori's research was the large number of patients who experience liver or kidney damage, causing 22.8% of them to drop the treatment. Several other studies have shown potential beneficial effects of remdesivir but suffer from the same design flaws.
Dr. Anthony Fauci did comment on a large clinical trial of remdesivir during a photo opportunity at the White House. Preliminary data was showing that the drug shortened the time to recovery by 31%. The study was published on May 22nd and did show a shortened time to recovery. Treatment with remdesivir did decrease the fatality rate but did not eliminate it, with 7.1% dying in the test group vs. 11.9% in the placebo group. Futher studies of remdesivir show that it does have a benefit, but its not clear if the difference was enough to be useful in a clinical setting. We need to keep searching for better treatments. A notable problem with all of these trials is the use of the drug long after the infection begins (often seven days), and frequently in critically ill patients. Other antivirals are known to work best if used early in infection. With more information being available in 2022, WHO now conditionally recommends treatment with remdesivir
Paxlovid (Nirmatrelvir and Ritonavir)
Pfizer in 2021 developed an effective oral treatment against SARS-CoV-2. Nirmatrelvir is a viral protease inhibitor that prevented the replication of the virus. Clinical trials of Paxlovid reduced the death rate by 88% in high-risk patients if given within 5 days of symptom onset. A second study showed a 70% reduction of hospitalization and no deaths in moderate-risk patients. Ritonavir is added to the medication to slow the metabolism of nirmatrelvir. This is a blockbuster drug against the virus and will prevent many deaths. However, over time the virus will likely developed resistance to Paxlovid and we need to keep searching for new drugs to treat the virus.
14 - 6 Vaccine development. How does it work?
The COVID-19 pandemic is not possible with the development of safe and effective vaccines. The goal of any vaccine is to create an immune response in the host that mimics a natural infection close enough to raise a protective immune response. Vaccines expose the host to enough of the pathogen to create this immune response without causing disease or any other life-threatening reactions.
The good news is that we have studied coronaviruses for years, which points out why basic research on seemly “esoteric” topics is essential. Ground floor research increases our foundational knowledge and often gives us a leg up in emergency situations such as this pandemic. Even more good news is that creating a vaccine against this virus should work. Go back and look at Figure 14-1. The prominent spike protein is a primary target of the immune response against the virus, and our immune system has an intense reaction against this protein that is protective. The current vaccines available for SARS-CoV-2 are amazingly effective.
Usually, the steps of vaccine development occur in three linear phases (Figure 14-5). Before clinical trials begin, experiments are performed in cell culture or animal models to demonstrate effectiveness. Phase 1 clinal trials then begin and involve testing the safety of a vaccine. An ideal trial will contain a control group that gets a placebo vaccine. These initial trials are typically small, using a few dozen people, intending to demonstrate no harmful effects of vaccination. The researchers also do experiments to measure the strength of the immune response and determine safe and effective dosing. Efficacy may also be looked at if enough participants end up contracting the pathogen. If researchers judge the vaccine to be safe, then more extensive phase 2 trials commence. A few hundred people, often a more diverse set, will receive the vaccine, again including a control group. Scientists follow participants in a similar fashion to the phase 1 participants and may compare different dosing schedules. Phase 3 trials involve thousands of participants but repeat the same steps, just with a large group. For a vaccine to proceed to production, it must demonstrate a protective effect against natural infection. These trials must take place in areas where the disease is currently spreading. One ethical concern when dealing with a deadly pandemic is the inclusion of a control group in the study. There are ways around this, but limiting the control group can make data harder to interpret. One possible solution is to run trials with multiple vaccine candidates that all share a single control group, allowing more subjects to get test vaccines.

Figure 14.5. Vaccine development timelines. In a typical vaccine pathway, each step proceeds only after a previous step shows promising data.(A) Due to the urgency of the current pandemic, many governments and companies are using a compressed timeline.(B)
The development of vaccines has several pitfalls. It is essential to determine what part of the spike protein is going to raise the most vigorous immune response, and this is simply not known. Scientists making the vaccines have to make their best guess and test it. Any mistakes will cause delays. We were exceedingly lucky with the SARS-CoV-2 vaccines because the scientists guessed right. There is also the possibility that a vaccine will make the disease worse. It could raise a robust immune response that doesn't stop the virus but increases the reaction in host tissues, such as the lungs — causing more damage. What scientists will be looking for is a highly neutralizing-antibody response, which is more likely to be protective. Another important parameter is how long immunity to infection will last? Life-long immunity is ideal, but any significant period of protection would likely be helpful. The vaccines turned out to not have negative side effects and all of them were nearly 100% effective at preventing death.
With those cautions firmly in your mind, I will say there is room for optimism. The development of vaccines for the current pandemic is proceeding at warp speed. As soon as China announced that a novel coronavirus was spreading host-to-host, and the sequence was available, companies and scientists working on MERS vaccines shifted gears and began to develop candidates for SARS-CoV-2. Because of the urgency of the pandemic, scientists and governments worked around the clock and used a compressed timeline for vaccine development. Compression is possible by overlapping some of the steps. Regulatory preliminary steps are occurring before results are known. Once data is available, rapid decisions are possible. Manufacture scale-up of promising candidates can begin before the completion of final trials to enable early production if all goes well. This compression is financially risky, but backup support from governments can remove that impediment.
Currently, there are dozens of efforts to create a vaccine, and they generally fall into four categories, nucleic acid vaccines, whole virus vaccines, component vaccines, and engineered viral vaccine platforms. In the rest of this section, I will give you background on how each method works.
Nucleic acid vaccines
Nucleic acid vaccines are a recent innovation in immune therapy. A person is injected with either DNA or RNA that, due to the vaccines' formulation, ends up inside host cells. The cell then synthesizes the proteins encoded in the nucleic acid. Since the entire set of viral proteins is not present, there is no possibility of a viral infection. However, the host cell degrades the foreign viral proteins synthesized, and portions of them appear on the surface of the cell. This display mimics what would happen in a real viral infection, causing their detection by the immune system, which will marshal a response. The hope is that this immune response will be strong enough to protect against a real viral infection. While this is a newer platform, developers and regulators do have experience with this platform from developing personalized vaccines against cancer.
Moderna's mRNA-based vaccine entered phase 1 clinical trial less than ten weeks after the first genetic sequence of the virus was released. The initial results of this clinical trial were encouraging. It is safe to use in people. Even more encouraging, it was able to raise antibodies against the virus at levels that are comparable to those seen in people that have recovered from COVID-19 infection. Tests of eight of the subjects showed they had a neutralizing effect on SARS-CoV-2. Also, challenge experiments in mice vaccinated similarly showed they had immunity to the virus and didn't get sick. The results of phase 3 trials showed the Moderna vaccine to be 95% effective at decreasing the risk of infection and serious disease.
Pfizer's mRNA-based vaccine was shown to be equally effective, and both were authorized for use. We have since learned that the vaccines have long-term protection against death; however, protection against infection wanes. The continued evolution of the virus, along with decreasing antibody levels in vaccinated patients, eventually makes them once again susceptible to infection. A vaccine that targets the site of replication, the nose, may have the ability to generate more long-lasting protection against infection.
Component Vaccines
Another approach to creating vaccines is to take just one small part of a pathogen, in most cases the part that the immune system can see and react to, and use that to create an immune response. For SARS-CoV-2, this will most likely be the spike protein, possibly supplemented with other proteins from the virus. Many conventional vaccines are component vaccines, including tetanus, diphtheria, pertussis, and pneumococcal vaccines. Thus, a known manufacturing platform is available to create a large number of doses quickly. There were nine such vaccines in development for SARS-CoV-2.
A significant concern with these vaccines is that it is not clear whether viral proteins alone will raise a protective immune response. An advantage of the other types of vaccines is that they more closely resemble a viral infection and elicit an antibody response and a cell-mediated response. Both of which may be necessary for protection against the virus.
Whole virus vaccines
Because the fastest vaccines out of the gate are novel, it is also necessary to continue developing more conventional vaccines. Whole virus vaccines involve using either a live, attenuated strain or an inactivated SARS-CoV-2 virus. These types of vaccines have a long, successful history of use in vaccine development. Inactivated virus vaccines require multiple doses and are slower to develop than nucleic acid vaccines. Attenuated vaccines take even longer than inactivated vaccines because it takes time to create a weakened version of the virus that is safe to use in humans. Several inactivated viral vaccines are progressing. The BBV152 vaccine manufactured and produced in India by Bharat Biotech has shown promise.
Whole-virus vaccines have the advantage of experience. Manufacturers know how to scale up successful candidates, and the infrastructure to grow them is already available. However, in both cases, large quantities of the virus will need to be grown to create enough doses for the world population, and this will take considerable time. Another advantage of these vaccines is their relatively robust nature for distribution in comparison to the mRNA vaccines.
Engineered viral vaccine platforms
A new approach that combines our knowledge of growing known viruses with the ability to include novel proteins is engineered vaccine platforms. These platforms use a known virus, such as the flu virus, that is modified to contain genes from a vaccine-targeted virus - in this case, the spike protein from SARS-CoV-2. The genetically modified flu virus is a self-limiting version of flu strains that replicates enough to cause a robust immune response, but not enough to cause disease. Yoshihiro Kawaoka and Gabriele Neumann, founders of the start-up vaccine company FluGen, were developing a new type of flu vaccine when the COVID-19 epidemic hit. Kwaoka's lab inserted gene sequences from SARS-CoV-2 into their vaccine candidate to create CoroFlu that should raise immunity to both viruses.
A key feature of this vaccine is its delivery into the nose, simulating the infection route of both viruses. CoroFlu then enters cells and begins viral replication. However, the essential M2 protein is missing from the virus, so it cannot escape the cells it infects. Instead, it elicits a hopefully strong immune response. The refinement of the vector and testing in animal models is expected to take three to six months. From there, the technology will be handed off to Bharat Biotech to manufacture CoroFlu and begin phase 1 clinical trials that could start as soon as the Fall of 2020.
If CoroFlu is successful, Bharat Biotech is capable of manufacturing 300 million doses a year. Given the urgency of the situation, the enlistment of other companies could provide enough for the world. CoroFlu is an untested, novel technology. It may be that a strong immune response against SARS-CoV-2 is not possible from this platform. An advantage of this method is that the infrastructure to grow large quantities of influenza virus is available, and the process is well known.
Another promising vaccine platform, invented at Oxford and being developed in partnership with AstraZeneca, is ChAdOx1 nCoV-19. Their vaccine uses an adenovirus that infects chimpanzees, but cannot replicate in humans. To this, they have added the spike protein from SARS-CoV-2. Since humans have never been exposed to this virus, they will not have a strong immune response against the vector. Thus antibodies will not neutralize the vaccine before the rest of the immune system can raise a strong immune response against the spike protein. Phase 1 clinical trials are now completed and published. A strong immune response against the virus was detected and shown to be able to neutralize the virus. AstraZeneca has received a $ 1.2 billion-dollar grant from the US for phase 2/3 trials that will enroll 30,000 participants in the US, 10,000 in the UK, 2,000 in South Africa, and 5,000 in Brazil.
This effort also succeeded, providing another weapon to use against COVID-19. The scientific team has experience using this vector in other vaccine trials. Infrastructure for growing the virus is already in place and can be scaled up rapidly to create millions of doses. Vaccine development will continue in all companies as boosters may eventually be needed against SARS-CoV-2.
14 - 7 Conspiracy Theories About COVID-19
The advent of the internet, web browsers and cheap content servers have made it possible for anyone to publish their ideas. In many ways, this is a beautiful thing, but it has a darker side. Someone with little expertise can present inaccurate, misleading, and dangerous ideas in compelling ways that may sway some individuals. This blind leading the blind can lead to tragic results. It's gotten so bad I wrote a whole chapter about the problem and how you can combat it. The COVID-19 pandemic is no exception and is fertile ground for numerous conspiracies. In this section, I will debunk the ones that I have come across. If you have found others, let me know, and I will add them to the list.
SARS-CoV-2 is an engineered virus created in a Chinese laboratory in Wuhan
The assertion that the Chinese released this virus from a lab has appeared in numerous publications that I refuse to list here and has been talked about by unscrupulous politicians and talk show radio hosts. Proponents of this theory suggest the virus was created in gain-of-function research to help understand SARS-CoV-2, and it happened to be released into the environment accidentally. Their proof of this theory is that there is a biosafety level 4 laboratory present in Wuhan China, and the lab had housed some coronaviruses. (BSL-4 laboratories work with some of the most dangerous pathogens) That's the proof. As you can probably surmise, being in the vicinity of an outbreak doesn't mean you caused it.
So what evidence is there that this is a naturally occurring virus? There is plenty. First, the sequence of SARS-CoV-2 is known. If you compare it to other known coronavirus sequences, you find it has a very high homology to coronaviruses found in bats. You can also trace its lineage through bats, into intermediary hosts, and then to humans. Second, an examination of the spike protein of SARS-CoV-2 shows that its adaptation to the ACE2 receptor in humans occurred by a different method than those previously predicted. In other words, scientists would not have known that this change in the spike protein would result in more efficient binding. If they didn't know the consequences of this change, how could they engineer the virus? Third, an engineered virus would have telltale artificial sequences that were leftover by genetic manipulations. These do not exist in SARS-CoV-2. It looks like any other natural coronavirus.
After being presented with this evidence, conspiracy theorists just moved on to a different claim. While the virus is naturally occurring, the scientists in the Wuhan laboratory isolated the virus and then accidentally released it into the general population. This idea also doesn't hold up very well. If they had isolated a natural virus that was capable of spreading human-to-human (i.e SARS-CoV-2), then it already was in the population, and it being in the laboratory would have made no difference. If it were an animal virus, isolated from a bat, it would not easily spread in humans. If it does, then we are back to my first point. There is no evidence that the Wuhan laboratory had copies of the virus before the outbreak started.
Finally, what difference does this argument make? Does it stop even one infection? Will it bring back anyone who has died? These blame games are just attempting to distract people from the urgent problems we need to address.
The death rate from COVID-19 is not accurate?
Due to the lack of testing and the inexperience of health professionals dealing with the pandemic, it is highly likely that the number of COVID-19 deaths is inaccurate. Some argue deaths are being incorrectly attributed to COVID-19, while others claim the current situation is leading to an undercount. To answer this question, the CDC did a study of excess mortality in New York City. At present (May 2020), NYC is the epicenter of the epidemic having thousands of active cases. The NYC health department previously developed an electronic vital statistics reporting system that provides a rapid and nearly complete count of all deaths in the city. Using this database, researchers were able to compare the all-cause mortality in NYC in previous years with mortality in the current year. By subtracting a baseline expected death rate, it is possible to calculate the number of excess deaths in 2020. From March 11–May 2, 2020, a total of 32,107 deaths were reported in NYC, which is 24,172 deaths above the expected baseline. Subtracting all reported COVID-19 deaths during this period leaves 5,293 excess deaths. Most of these are probably due to COVID-19, but not all. Some may be from patients who fear to or could not seek medical attention due to the epidemic, but were not infected with the virus (for example, someone having a heart attack). A large number of excess deaths is compelling evidence that health departments are underestimating the death rate from the epidemic by up to 22%.
You can get COVID-19 more than once
There have been numerous news stories discussing the possibility that someone can be infected with SARS-CoV-2 more than once, suggesting that humans do not develop immunity to the virus. It is true that some people who were infected, then tested negative for the virus, and later were found to later test positive again. Some people worried this meant that they had been reinfected. Recent research by Chandrashekar et al. in monkeys has definitively demonstrated that vaccination or natural infection by SARS-CoV-2 provides immunity to reinfection. Monkeys are not humans, so it is possible, but unlikely the results would be different in humans. Also, the South Korea CDC reports that humans who tested positive a second time did not pass the infection on to others.
In reality, these second positive tests probably have more to do with the extreme sensitivity of the test. The RT-PCR tests for SARS-CoV-2 don't detect the live virus. They signal the presence of the RNA of the virus. Because PCR exponentially amplifies its target sequence, it is exquisitely sensitive, being able to detect just a few copies of SARS-CoV-2 in a sample. What these retests are probably identifying is leftover garbage RNA from the virus that the immune system hasn't cleared out. There is no live virus. Reinfection may be possible. In these cases, a person's immune system would deal with the virus, would not develop severe symptoms, and would not pass the virus on to someone else.
However, about six months after infection, due to waning immunity and evolution of the virus, subsequent infection with SARS-CoV-2 is possible. The variant will often be different. Because of previous exposure to the virus, the second infection is often milder than the first infection. Those with the best protection are vaccinated with boosters and have been infected with the virus. Almost as effective are those who have had all their vaccinations. Subsequent infection without vaccination gives the poorest protection against future infections.
Stay-at-home orders don't work and are the government's way of getting us used to their control
When an epidemic begins to spread in a community, an age-old practice is to separate sick individuals from the general population. During the plague outbreaks of the middle ages, you would be put into small rooms and locked in. The family would give you food and water as needed, but you would not be allowed out until you were recovered or dead. In the 18th century, practices were somewhat more humane. Camps or pest houses kept ill members of the community away from others. This type of quarantine was somewhat useful but created the problem of caring for sick individuals and was also used to discriminate against the poor and minorities.
In the modern battle against COVID-19, governments are using a mixture of self-quarantine at home, and dedicated hospitals to house individuals struggling with the disease. In places where the spread of SARS-CoV-2 has become out of control, or where adequate testing and contact tracing were unavailable, states and nations issued stay-at-home blanket orders to try to decrease the spread of the virus.
As these stay-at-home orders have dragged on, there has been growing resistance to them. If someone's employment is deemed a non-essential service, they were unable to work. According to a report on Americans' economic well-being, about 40% of the US population would not be able to cover a $400 emergency. These stay-at-home orders put these folks in an impossible situation. If these workers go to work, they risk their lives and their families, but if they cannot, they don't have enough money to survive. The response to this crisis by the Federal Government has been inadequate, leaving many of these people desperate and claiming that stay-at-home orders are an overreaction and an impingement on their freedoms. To help people abide by these rules, it is essential to know if stay-at-home regulations work.
One of the best ways to understand how a disease spreads through a community is to use software that can realistically model an epidemic's spread and then allow you to manipulate parameters and see what happens. Malia Jones, an epidemiologist at the University of Wisconsin-Madison, has taken the time to create a game that a novice can use to understand these concepts. I encourage you to play with the model. I hope you realize after experimenting that it's likely that social distancing works. But are there any real-world examples?
The COVID-19 epidemic is not the first time that governments have used social distancing. During the last great global pandemic, the Spanish flu of 1917-1920, many municipalities closed schools, quarantined victims in their homes, and banned large gatherings to prevent the spread of the disease. Because cities reacted at different times and in different ways, it is possible to compare their responses and observe what appears to work best. A study in JAMA shows that if these interventions are started early enough and last long enough to bring case levels low enough, propagation of the virus stops. Philadelphia had its first case of influenza on September 17th, 1918, and campaigned against coughing, spitting, and sneezing in public. Inexplicably, ten days later, city officials hosted a parade that 200,000 people attended. Eight days after their death rate began to increase, and social distancing orders were put into place. However, it was too late, and the death rate ended up being 748 per 100,000, one of the worst in the country.
In contrast, two days after St. Louis experienced its first case of influenza, it implemented strong social distancing orders and kept them in place for six weeks. As a cautionary tale to current state governments, some cites relaxed social distancing before the case rate had decreased significantly, causing a second spike in cases and a reimplementation of social distancing for another five weeks. In the end, St. Louis had a death rate of 358 per 100,000, less than half of what Philadelphia experienced.
The message from these studies is clear, in the face of no drug treatments and no vaccine, social distancing is our best option to decrease the spread of COVID-19. If governments implement these measures soon enough and hold them long enough, social distancing slows the spread of disease and reduces the overall death rate. However, these measures do not solve the problem of the suffering of so many Americans who are now out of work. Our government needs to do a lot more to help these people.
Anthony Fauci and/or Bill Gate will profit from remdesivir
This rumor is so ridiculous I am not going to spend much time on it. Dr. Fauci is the director of the NIAID (National Institute of Allergy and Infectious Disease) and is an infectious disease expert. He was appointed to the post in 1984 by Ronald Reagan and has served under both Republican and Democratic Administrations. Bill Gates is a co-founder of Microsoft, and part of his philanthropic efforts have been in vaccine development. For the current crisis, Mr. Gates' foundation, along with other groups and governments, started the Coalition for Epidemic Preparedness Innovations in 2017. CEPI is helping to organize vaccine efforts and is helping manufacturing facilities to prepare to make whatever vaccine turns out to be effective.
Remdesivir is a drug developed by Gilead Sciences, initially as a potential treatment for Hepatitis C, and later was investigated as a treatment for the Ebola virus. Recent testing against SARS-CoV-2 has shown it may be clinically useful. Neither Dr. Fauci nor Mr. Gates has any investments in Gilead Sciences or any other known conflicts of interest.
The various vaccines against COVID-19 will make you magnetic, will implant a chip, will make you sterile, and are more dangerous than the disease
Seriously? Do I really need to even address these rumors? I can tell you from personal experience that getting vaccinated does not make you magnetic. No metal sticks to me. There are no chips present in the vaccine, and honestly, you are already being tracked because you carry your mobile phone with you wherever you go. Who needs to implant a chip in you? Make you sterile. No, no, no! Just because you read it on the internet doesn't mean it's true. Go back and read Chapter 2 of this book. While it is true that some people who have received the vaccine have died, that doesn't mean they died from the vaccine. When you vaccinate millions of people, some by chance are going to die within a few days of getting the vaccine. If you compare the rate of death of people who have received the vaccine to those who have not, the rate of death is the same. Thus, the vaccine is not the cause of death.
14 - 8 A call to action: what you can do to fight this epidemic
I hope this chapter has helped you learn more about SARS-CoV-2 and the disease it causes. Even in the best of circumstances, COVID-19 was going to be a long, hard fight. All the frightening news stories can leave one feeling powerless against this disease. But that was not the case. We are on a way to beating it There is a lot you can do to help. Many of this advice is no longer needed in some parts of the world, but I leave it here as a reminder. And maybe for the next pandemic, which I hope is many years in our future.
- Get vaccinated. The death rate from this infection is at best 0.5%. That seems small, but since we think that the entire world population is susceptible, that's over 35 million people! If enough of us get vaccinated we can stop this pandemic and protect those around us.
- Wear a mask to prevent spreading the COVID-19 to others. A recent paper in Nature indicated those ill with coronavirus will shed droplets containing the virus into the air. However, if the person wore a surgical mask, virus in droplets were undetectable. Other studies have shown that even masks made out of T-shirt cotton are 70% effective at blocking particles. This is so important because initial infection with SARS-CoV-2 is asymptomatic for around five days, yet the infected person will be shedding virus. For some reason, this has become a political statement and a sign of bravery, which is ridiculous. Avoiding wearing a mask is not brave; it's selfish.
- If you are ill, self-quarantine. In the outbreak in South Korea, a COVID-19 (+) patient was asked to self-quarantine, but ignored those rules and went to a church service. Her carelessness became a super spreading event initiating thousands of other infections. Stay home if you are sick! And please, continue that behavior after this epidemic is over. This one drives me nuts. In American society, it is somehow laudable to soldier on even if you are sick. Unfortunately, many workplaces offer no paid sick leave, making staying home for many impossible. This absurd predicament is not only cruel, but it also decreases productivity and increases employee turnover rates.In other words not providing paid sick leave to your employees is penny wise and pound foolish. You are losing money.
- Listen to your national, state, and city health departments and do what they ask. If we follow local social distancing guidelines, we can significantly reduce the transmission of COVID-19.
- The next two suggestions are a bit off the wall, but the science seems reasonable, if untested. Take vitamin D. Studies with influenza have shown that vitamin D supplementation reduced the risk of influenza. Vitamin D deficiency has been linked to acute respiratory distress syndrome, a complication of COVID-19 that is one of the most serious. I would like to see more supporting evidence showing vitamin D supplementation does make a difference for COVID-19.
- Using mouthwash could reduce the transmission of SARS-CoV-2. A study in Function by O'Donnell et al. reasons that since SARS-CoV-2 is an enveloped virus, meaning a membrane surrounds the viral RNA, a mouthwash that disrupts that membrane would reduce the viral load of infected individuals. They point to other studies with influenza and other coronaviruses that demonstrate the effectiveness of this approach. Again, more work needs to be done on SARS-CoV-2 to show mouthwash works. But, even if it doesn’t work, you breath will be much fresher.
- Stay calm and act rationally. In the wake of the social distancing orders and the beginning of the outbreak in the US, people were afraid. In response to that fear, they purchased a large amount of toilet paper and bottled water. That was not necessary.
- The good news is that our cooperation as a society does not have to be perfect. If about 70% of the population does what is necessary, we can beat back COVID-19. Or course, the more cooperation we have, the faster we get there.
One thing this epidemic has shown everyone is that we need each other. The doctors, nurses, and caregivers are there to treat all those sicked by the illness. Farmers grow food year-round, and food processing plants turn that into the products we consume. Truckers, railway operators, US postal workers, and all the others in the transportation industry get the food and supplies we need to their destinations. Grocery store workers stock the shelves and help us to get the food we need. And do not forget the police and firefighters who are still on the job to keep us safe. Without all these essential employees, society would not function. It's a little ironic that these occupations are some of the lowest-paid positions. They should not be!